

#287: Google's big swinging distribution mechanism enters the AI race
The one-minute (ish) healthtech roundup, by SomX.

Hello healthtech fans.
This week: Google have slapped their health coach on the table and a clinical AI startup wants to wrap it up.
🎙 Fancy this newsletter in podcast form? 👇 Well… Click this linky link to get the pod on Spotify. And it’s on the SomX YouTube channel if you like to look at the faces of people when they talk.
News Bites 🥪
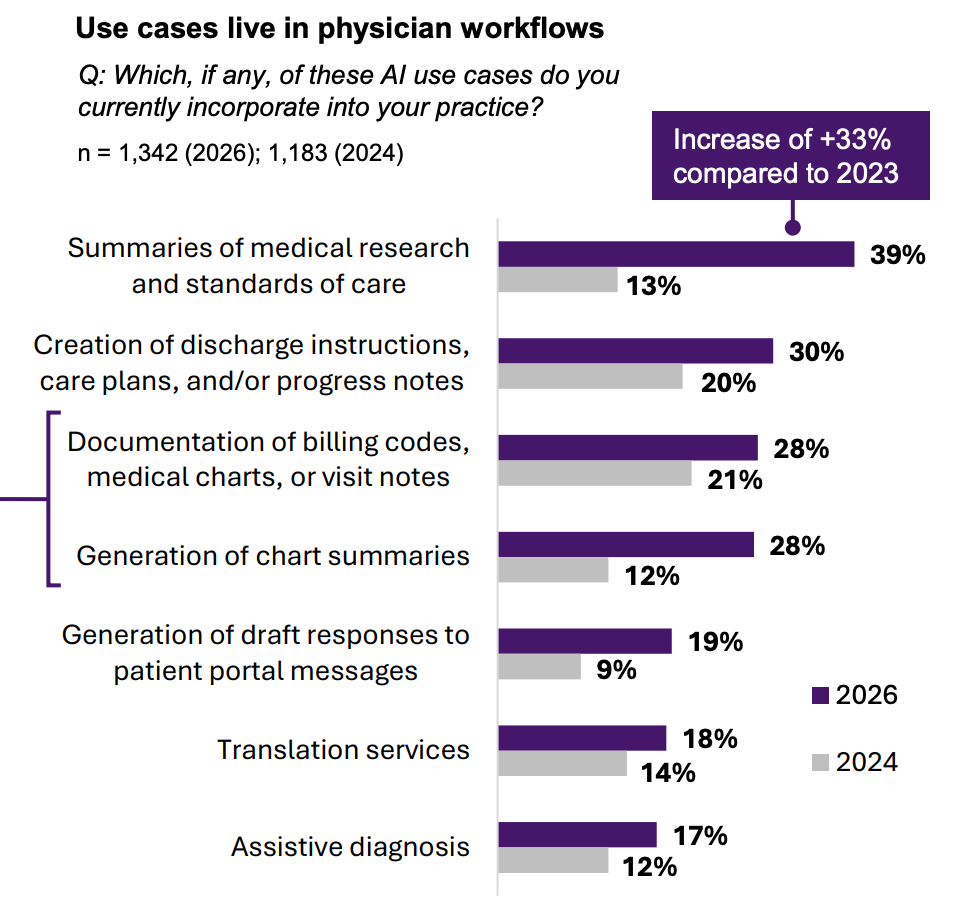
📊 8/10 doctors now use AI. They just don’t want their patients to: Rage-baiting you with that headline to make a point… I removed all the context and went for an emotional reaction… did it work? The survey is from the US and shows a big jump (38% to 81%) of clinicians using AI in their work. Before you panic, take a look at the graph below for what they’re doing with it. When you talk really broadly about ‘clinicians using AI,’ it’s incredibly easy for your mind to go straight to diagnosis and treatment. The reality is very different. Assistive diagnosis was just 17% and even that should be broken down into exact tasks before we cast judgement. Why? because here’s two prompts that may require Class II device certification, but have wildly different safety profiles:
“Based on this history and examination, have I missed anything in this differential diagnosis” is very different to…
“What treatment shall I give for a patient with leg pain and PR bleeding.”*
🧠 Forget making LLMs better at therapy. Wrap a clinical brain around them: Instead of expecting OpenAI, Anthropic, Google, Meta to become compliant or better at therapy (one of the most common applications of LLMs since their inception), could we think of it a different way? Limbic just published a randomised, double-blind trial in Nature Medicine showing that their “Limbic Layer,” a clinical reasoning system trained in CBT, when wrapped around general-purpose LLMs like ChaGPT, Claude etc., produced therapy sessions rated superior to bare LLMs AND to human clinicians on standard CBT scoring metrics. There was also a ‘complimentary’ real-world analysis of nearly 9,000 users and those with highest exposure to the Limbic Layer had a 51.7% recovery rate versus 32.8% in the comparison group. The question is what now…**
💷 £7.4bn for NHS digital. Now someone just needs to spend it well: This is the number the healthtech market has been waiting to see. DHSC and NHSE’s internal plan commits £7.4bn to technology, digital and data through to 2030. It won’t directly unblock the commercial dry spell, but if it’s spent well and fast, the procurement pipeline should follow. Big if. Also, to be absolutely clear, this is internal planning guidance, not a spending announcement, so don’t go refreshing the tender portals just yet.
🤰 Nadia Care raises $12M to bring maternal care back to the community: They’re expanding a community-based maternal health model across the US. And get this, tech fans… Their approach is deliberately low-tech in places - care actually delivered at home, virtually, and yes, Walmart car parks. The round was led by Valtruis and a national payer, which suggests someone believes the unit economics work. The maternal mortality crisis, especially for Black women, is one of the clearest failures of the healthcare system, so you can’t ignore results like this… 60% drop in NICU days, 47% reduction in low birth weight, and 38% fewer preterm births across roughly 4,000 members since 2021. Deserves more than $12M.
🫀 CT-like chest imaging at the bedside sans radiation: “If it sounds too good to be true, it probably is.” That’s the type of phrase that motivated engineers at the University of Hong Kong to prove you wrong and develop SonoMeta***, which, granted, isn’t CT, it’s AI powered ultrasound (cool name though - Metalens), but it uses metamaterials that can visualise cardiac structures up to 10cm behind the rib cage - that’s approaching CT quality and get this… Zero radiation. And at the patient’s bedside. It’s currently in multi-centre clinical trials in Shanghai and Hong Kong and the obvious application: emergency settings, ambulances, anywhere you’ve ever thought - “if only we had a CT and we could do X.” Commercially very compelling if the trial data holds up.

🧬 Roche builds pharma’s biggest AI factory: Roche has gone full send on AI infrastructure, announcing a massive expansion that brings its total on-premises GPU count to over 3,500 NVIDIA Blackwell chips - the largest announced GPU footprint of any pharmaceutical company. Here we go… some fun stats… At around $30–40k per GPU, we’re talking somewhere in the region of $125m on chips. Also, at (allegedly****) 84% gross margins on each chip, Jensen Huang is the real winner. The Roche vs NVIDIA partnership stretches back to 2023, and Roche says the “AI factory” powers its Lab-in-the-Loop approach, where AI models and wet-lab experiments feed into each other at scale.
🧠 Blood test spots brain tumours with 90% accuracy - works like a Covid test: UK scientists coming up clutch this time at the University of Manchester - they’ve identified a pair of blood proteins that can detect glioblastoma with 90% accuracy. It’s in clinical trials across six UK sites and four internationally, and the team wants to expand it to cover other brain tumour types too. Exactly the kind of diagnostics innovation we need more of. The “within a decade” timeline is promising and optimistic. But if it works, genuinely transformative.
And finally...
🏋️ Google wants Fitbit to know your medical history. Sure, why not?: This was coming wasn’t it. Google’s upgrading Fitbit’s AI health coach to integrate with your medical records. They were first out of the gates with consumer health AI, then watched OpenAI, Anthropic and Microsoft lap them on the underlying models. Many people are expecting Google to win the AI game and here they come with their big, swinging distribution advantage (Fitbit’s enormous installed base) to get back in the race. Would you trust a wearable brand with your medical info, though?

What to listen to 🔊
I spoke to Ian Wharton of Aide Health this week - fascinating one that a lot of founders and healthtech product teams can learn from around how design influences and shapes so much of product’s success in healthtech. Only 3-4% of patients stick with health apps after 30 days and Aide hits 70% at three months. We get into conversational AI, medication adherence, and why a six-person startup is pursuing Class II regulation.
How do you actually sell innovation into the NHS? Tara and Jim explore the reality behind commissioning, the strategy, relationships and science that turn good ideas into funded services. One of the biggest takeaways? Innovation doesn’t fail because the idea isn’t good, it fails when funding, decision-makers and system priorities don’t align. Listen to this for practical info on going from concept to commissioned reality.
What’s Updoc? Hilarious joke and exactly what you find out the answer to on this episode with Pete. They get into how they're reshaping primary care access for rural and time-poor patients - streamlining intake, triage and workflow while keeping clinical governance tight.
Events 📅
HealthTech & Wellbeing Tech Meetup
📅 19th March
🇬🇧 27 Euston Rd, London
A practitioner-level conversation about AI, investment, and the real state of HealthTech and Wellbeing Tech.
Clinical Product Drinks #002 🍸
📅 25th March
🇬🇧 41 Gracechurch St, London, England
Clinicians, product people and healthtech builders convening for drinks in the City. If you work at the intersection of healthcare and product, this one’s for you.
Healthcare Conference 2026 – The Longevity Frontier
📅 30–31st March
🇬🇧 London Business School, London
LBS brings together healthcare leaders to discuss longevity and its impact on healthcare systems. Worth a look if you're thinking about what the ageing population actually means for the sector.
Opportunities 🕵️♀️
🔍 Data Science Team Lead - Elsevier: Elsevier is building AI-powered discovery tools for clinicians and researchers (think ClinicalKey AI, RAG systems, semantic search). They need a senior data scientist to own the search and evaluation roadmap. Meaty technical role at genuine scale.
🏛️ Scientific Adviser (AI in HTA) - NICE: NICE wants someone to lead AI integration into how it evaluates health technologies, one of the most consequential healthtech roles in the UK right now. If NICE gets this right, effective treatments reach patients faster.
🩺 Clinical Director - Heidi Health: Heidi (AI clinical documentation, 10M patient visits/month, $96.6M raised) is hiring senior clinicians or CMO-types to lead enterprise expansion across Europe. Big networks required; big opportunity in return.
💊 Clinical Operations Lead - Numan: The UK’s leading digital men’s health platform: diagnostics, medication, and clinical care across men’s health and obesity, needs someone to help scale clinical services across a 7-day model. Fast-paced, already at scale.

📣 NIHR Survey: Why Aren’t More Medical Technologies Designed for Children: Only 0.5% of FDA-approved orthopaedic devices were designed for children. Just 2% of approved AI radiology tools are labelled for paediatric use. Only 5% of the UK’s national research budget goes to paediatrics. The NIHR HealthTech Research Centre in Paediatrics and Child Health wants to understand why - and they need to hear from industry. If you work in healthtech or medtech (even if your focus is entirely adult populations), this short survey is asking what the real barriers are to building for children and young people. The data will directly inform how the gap gets addressed. Takes five minutes. Worth it.
James’ editor notes
* Went for something random here to make the point that I don’t think clinicians (ignoring outliers) will ask AI to go from history to treatment in one go, especially for serious symptoms. Even in comms and marketing at SomX we say ‘shrink the task’ for AI as much as possible so that you don’t get errors on errors on errors carried forwards with AI doing multiple things and making multiple assumptions, and the human can then keep the train very much on the tracks. Where clinicians are prompting AI, OK it’s not a medical device and shouldn’t be used as such, but in the first example I gave, it’s checking if something’s been missed based on a full history, examination and documentation and any information it gives is going back through the human filter… it’s a much smaller task, and imo, a safer application. Being my own devil’s advocate, the issue then comes in how practice changes down the line, as a result. If you can rely on AI to check if you’ve missed something, do you change the way you take the history, examine, document? The answer is yes, so there’s lots to think about, but the nuance and detail is more important than rage bait headlines.
** If you want the down-low on how Ross (founder and CEO of Limbic) went about building clinical AI for mental healthcare, check out part 1 and part 2 of his episodes on The Healthtech Podcast. It’s fascinating.
*** Very unlikely to be true. Their motivation is not documented and has been assumed.
**** https://siliconanalysts.com/analysis/nvidia-b200-blackwell-cost-breakdown
📣 Want something in front of our 7,500+ readers?
You can break your news as the main story, feature a podcast, job or event... and we even have a few sponsorship packages to choose from...
We review everything editorially - if it is not right for our audience, we’ll let you know - everything has to be valuable to this glorious community.
See you next week, Pigeon fans ✌🏼