

I was afraid of AI reaching mental healthcare and I was wrong.
This is what I learned after putting the work in.


A note before we start. This piece deals directly with suicide, self-harm and severe mental illness, including details from a specific case involving a young person’s death. If that’s difficult territory for you right now, please look after yourself and come back to this another time. If you’re struggling, the Samaritans are on 116 123.
And, for transparency, I have no commercial conflicts to declare on this one. None of the companies named (Limbic, ieso, Ranvier) are SomX clients or compete with any of our clients, and nobody has paid for, sponsored, or seen this publication before. The companies appear because their founders came on my podcast and the work is genuinely fascinating and a frontier in healthtech that I want to talk about.
Half of NHS Talking Therapies patients don’t recover. That’s a strange thing to say without urgency, isn’t it? But we do.
At the last count, 50.2% of patients who completed a course of talking therapy came out of the other side recovered (which, by the way, was the target). Now there’s a new target of 53% by 2028–29, which the system is proud of working toward, and would mean… let’s just say it out loud… that a national achievement three years from now will be that 47% of mental health patients still don’t get better.
It’s hard to imagine any other clinical specialty setting that target. It’s actually impossible to imagine that. Why are we ok with mental healthcare not being effective for half the population?
And why doesn’t it work? Do we know who needs what, whether the therapy they got was any good, whether they actually got better? And what’s happening now, [trigger warning] when 1.2 million people a week are expressing suicidal ideation to ChatGPT (that would’ve read as hyperbole a year ago, and which is, in fact, OpenAI’s own published number)?
What looks to be finally forcing a change is technology, which the sector (myself included) spent the last couple of years being most afraid of. Not because AI will be scaled up to deliver therapy (that’s a different argument/discussion and I’ll come to that later) but because for the first time in the history of the specialism, the conversation generates a record, the record generates data, and the data makes the guesswork visible.
Historically, mental health has involved a fair amount of… well… guesswork. That’s hard to actually say out loud and, by the way, I’m used to an industry that uses sensationalist language for fun (and commercial gain), so I don’t take joy in ever doing that. But hear me out and I’ll try to explain.
A Likert scale in a stressed waiting room

The standard way to diagnose depression in UK primary care, in 2026, is to ask the patient to score nine statements between 0 and 3 on a form they fill out in a waiting room, often having just disclosed to a GP for the first time that they’re struggling. That’s called a PHQ-9. It broadly determines whether they get talking therapy, antidepressants, both, or neither, and which kind.
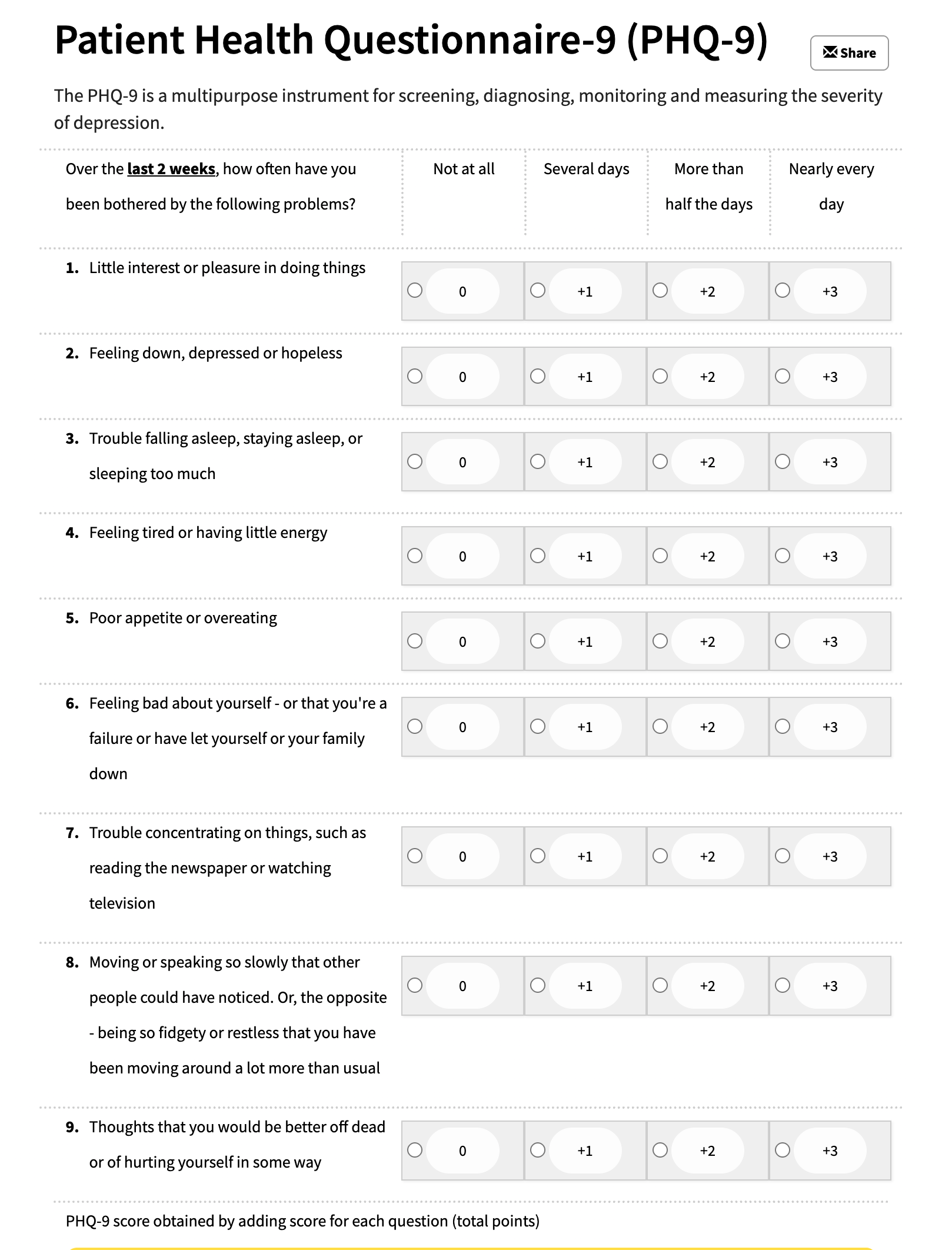
Now, indulge me, imagine the cardiology version. “We’re going to ask you nine questions about your chest, and then decide between an angioplasty and a triple bypass.” Yes, it’s not a direct comparison, but you get my point. Putting a subjective layer of patient reporting between the biological signal and the diagnostic input is far from ideal. That’s actually many layers of input and output influenced by the physical and metaphysical.
Ben Finley, who I had on my podcast recently (came up via Medtronic, drug development, and Publicis, now an advisor to Ranvier, a biotech company looking at new biomarkers for mental health conditions) put it pretty directly:
“We’ve normalised the guesswork in mental health in ways that wouldn’t be acceptable in any other field of medicine.”
Now, skilled clinicians and patient-advocates may argue that the patient reported signal is the signal and that the subjectivity and subsequent answers are actually to be interpreted. In part, I agree, and I fondly remember my liaison psychiatry job really honing those history taking and interpretation skills to find the real signal. I also remember a pain consultant who once said to me “if a patient communicates pain, they are in pain,” which stuck with me in medicine and in life. But at the same time, I don’t think Ben’s wrong either. Objective biomarker measurements plus patient reported symptoms is, frankly, a much better data set to inform diagnosis and track recovery.
But we’ve never had those biomarkers. There’s no biomarker to depression like troponin is to an MI. The patient’s own self-report on appetite, sleep, mood scores and others are, historically, all we’ve had.
The good news is that this is all changing in two places at once. The earlier-stage version is the work coming out of David Nutt’s lab on serotonin taste sensitivity as a surrogate biomarker, now being commercialised by Ranvier. You did, indeed, read that right, they’re creating an actual taste test for mood (you taste less-well in a depressed state). Whether that specific product makes it through trials or not, let’s agree that the direction is interesting and exciting, i.e. towards objective, measurable, biochemical correlates of mental state. It looks like we’ll get there in the next decade.
How is technology helping?
For context, let’s take a typical NHS Talking Therapies diagnosis. The patient has waited weeks for a phone assessment. The phone rings on a Wednesday afternoon. The clinician (overstretched) has fifteen questions to get through. The patient, who hasn’t said any of this out loud before, has to organise their whole life into the right slots in the right order before the clinician can decide which pathway they belong on. About half the time, they end up on the wrong one. Three sessions later, the new therapist works out the diagnosis was wrong and they get moved.
Now picture the newer version (with technology that’s been deployed across 45% of NHS Talking Therapies services). The patient self-refers at 2am on a Tuesday, when they’re actually willing to talk about it. They have an hour, not ten minutes, and they’re talking to a system that has read the entire clinical literature on the differential diagnoses they might be presenting with. A clinical reasoning layer behind the chatbot (crucially, not the chatbot itself, which matters, and I’ll come back to) predicts the right pathway. Published in Nature Medicine on 129,400 patients across 28 NHS services, the downstream pathway changes drop by 45%. And diagnostic reliability across depression, PTSD and generalised anxiety hits 93%. See references at the end.
NICE looked at this last year, cautiously. Much of the evidence base is company-produced. There’s an open question about what happens to people triaged out of services entirely. Both fair, both resolvable. The point is that mental health diagnosis has stopped being a thing only a human can do and started being a thing a machine can do reliably enough to be class-2A regulated.
It’s important to note here that I’m on record saying that “AI should never be placed at the point of human suffering, alone.” That position was based on a romanticised version of what I’d want healthcare to be. I’m a clinician at heart, my bias toward humans is obvious, but don’t we all want a human to care for us? Well, maybe, but that position turned out to be indefensible against the backdrop of people getting no support at all. I was oddly stubborn for a tech evangelist, but hey, I learned new information and changed my mind. I’d be interested in your views once you’ve learned what a clinical reasoning layer is too (coming shortly in this piece).
The therapy nobody watched
The second guesswork problem might be the most structurally awkward of the four, and I’m not sure I’ve fully worked out where I sit on it.
